Newsletter
No Surgical Items Left Behind
Apr 29, 2024
A missing sponge. A lost surgical needle. A post-op item count that doesn’t match the pre-op. One of the most critical and avoidable surgical errors is leaving a surgical item behind in a patient. What is known as a “retained surgical item” is classified as a “never event” by the Joint Commission due to the severe effects it can have on a patient, such as organ damage, infections, and even death.
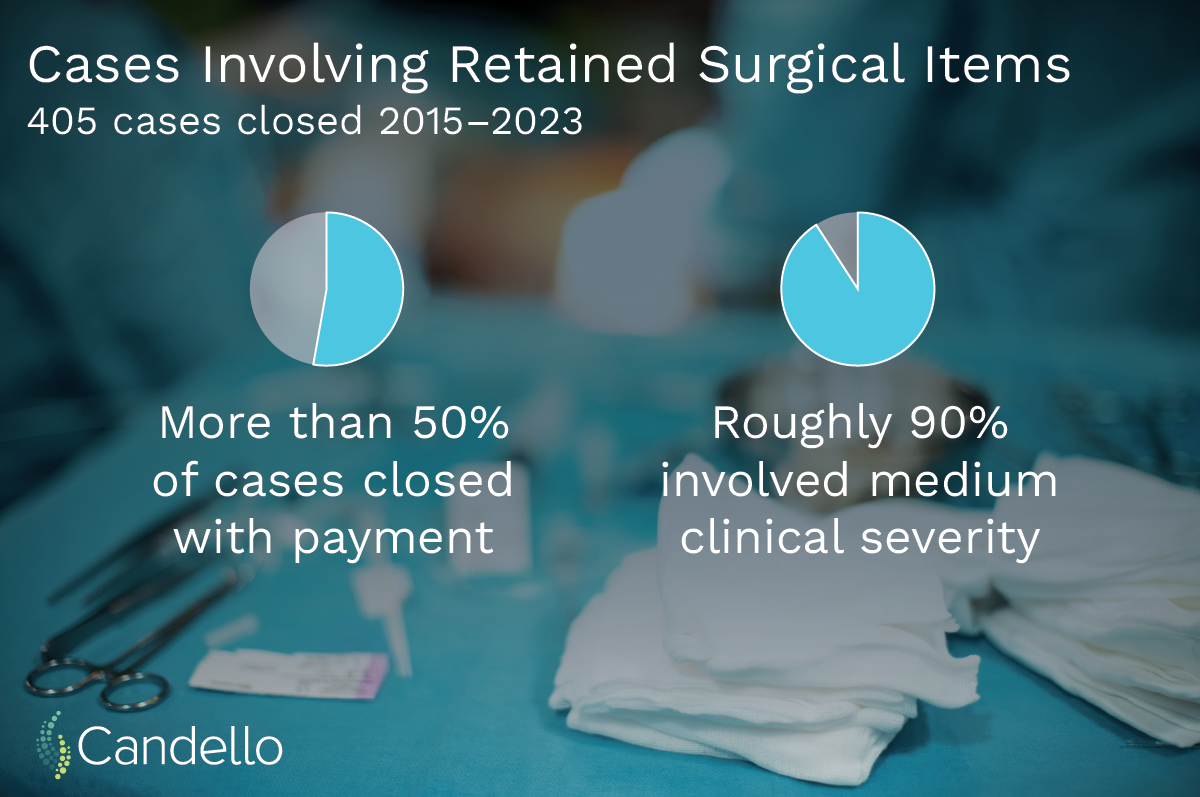
While the occurrence is rare, Massachusetts reported rising rates of retained surgical items over the past several years compared to pre-pandemic levels. The Candello database also contains 405 closed cases involving a retained surgical item between 2015-2023. The outcomes among these cases remained relatively steady, with more than 50 percent of cases closing with payment and roughly 90 percent having medium clinical severity.
Several members of the Academic Medical Center Patient Safety Organization (AMC PSO) convened a task force of surgeons, anesthetists, surgical nurses, and surgical technologists to analyze key contributors and suggestions to mitigate risks.
The task force recognized that the surgical item count is a vulnerable point in surgical patient safety. As part of standard surgical practices as well as the WHO’s Surgical Safety Checklist, the responsible team member verbally confirms the instrument, sponge, and needle counts with the surgical team before the patient leaves the operating room. However, identifying a count discrepancy is easier said than done, and the Radiological Society of North America found 88 percent of retained surgical item cases reported a correct item count.
The group of experts came to a consensus that distractions, shift changes, and problems with relationships and trust were the biggest contributors when it came to count discrepancies.
To help lessen interruptions during a count, the task force suggests asking the operating surgeon directly if they are ready for the count, announcing to the room that the count is about to start, and avoiding performing the count during critical times, such as shift changes or during anesthesia induction.
In the event of hand-offs and shift changes, the experts stress the importance of ensuring everyone knows their respective role in the operating room and who is responsible for the count.
Mitigating the risk of ineffective relationships and trust is more nuanced and requires a certain level of psychological safety among team members. For example, hierarchical structures in the OR may make a team member hesitant to voice their concerns. To address this challenge, the PSO discusses the benefits of crew resource management (CRM) training as well as simulation training for surgical teams.
Trying to prevent a count discrepancy is just one piece of the puzzle; some of the most critical patient safety moments are what happens when a count discrepancy occurs. The task force supports the steps provided in the NORC guidelines:
- Stop wound closure if the patient’s condition permits.
- Alert the entire surgical team and conduct a recount.
- Perform a thorough cavity search for the missing item(s).
- If there is still a discrepancy, search the floor, garbage, and linen, and if found, repeat the count to verify.
- If the count is still incorrect, perform an intraoperative X-ray and, if available, use a surgical wand, also known as RFID (Radio-Frequency Identification Device) to help locate any missing item(s).
The prevention of retained surgical items requires a comprehensive approach, including effective communication, standardized protocols, technology, and a culture of continuous learning and knowledge sharing.
Clinician Corner
As featured on CRICO’s Safety Net podcast, Douglas Smink, MD, MPH, General Surgeon at Brigham and Women’s Hospital and advisor for the retained surgical item PSO, shares his insights about developing the patient safety alert:
“We were aware that best practices had been published, but given the continuing occurrence of these events, thought that there might be some barriers or ongoing challenges and thought that was worth convening subject matter experts to really think about the patient safety risks and develop risk mitigation strategies specifically focused on operationalizing best practice guidance.”
You can download the full Patient Safety Alert here.
Additional Material
- Retained Surgical Items: How Do We Get to Zero? (Joint Commission Journal on Quality and Patient Safety)
- Cracking the Code to Prevent Retained Surgical Items (Outpatient Surgery Magazine)
- Retained Surgical Items (Association of periOperative Registered Nurses)
- Alert on Surgical Items Left Behind in Patients (Safety Net Podcast)
- Case Study: Communication Issue Leads to Retained Foreign Body
Recent Issues
Safety Nets for Safer Care

Recently Asked Questions
Why Went Wrong