Newsletter
At the End of Information Blocking, an Opening for Patient Safety
Mar 29, 2021
Patients gained instant and broader access to their health information, starting April 5, 2021. What will be the impact on patient safety and medical professional liability (MPL)?
The information blocking (aka “open notes”) rule of the federal 21st Century Cures Act dictates that eight categories of clinical notes created in an electronic health record (EHR) must be immediately available to patients through a secure online portal. Individual or organizational health care providers may not block, or delay patients’ access to, any eligible information (including test and studies results) entered and stored in their EHR.
Patients’ right to access their records were codified, under HIPAA, in 1996; the 2016 passing of the Cures Act legislation aimed to make access easier and virtually unrestricted. Specifically, the final rules of the Act require that patients have immediate access to the following eight categories of clinical notes:
- Consultation notes
- Discharge summary notes
- History and physicals
- Imaging narratives
- Lab report narratives
- Pathology report narratives
- Procedure notes
- Progress notes
Exempt from unrestricted access are notes “compiled in reasonable anticipation of, or use in a civil, criminal or administrative action or proceeding” and psychotherapy session notes. However, other components of psychiatric care (e.g., diagnoses, medications, appointment times, etc.) may not be blocked.
Impact on Safety and Liability
Opening your notes offers the potential to enhance patient safety by linking clinicians and patients between visits–times when ambulatory vulnerabilities often compound. Such a link may help detect and prevent errors by mitigating missed follow-up appointments and referrals, uncompleted diagnostic tests, delayed notification of abnormal test results, and persistent but undiagnosed symptoms. It may also provide a new platform for patients to report possible errors in their notes.
What was or was not documented is rarely the primary reason a patient files a claim or suit alleging malpractice, but the medical record is, essentially, the “key witness” in such proceedings. Any issues with that record (gaps, ambiguity, insensitivity) serves to undermine the defense of standard and appropriate medical care and has the potential to create an impression of negligence.
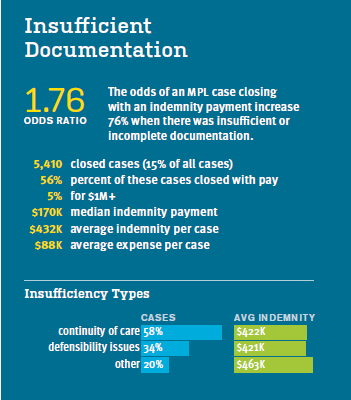
CRICO’s 2020 Report, The Power to Predict (based on data from CRICO’s national Comparative Benchmarking System), notes that the odds of an MPL case closing with an indemnity payment increase 76% when there are indications that documentation of patient encounters and care was inadequate to ensure appropriate care by subsequent caregivers, or to guide the patient’s involvement in his or her care decisions. From 2014–18, 56% of 5,410 cases with insufficient documentation closed with indemnity (compared with 30% for all MPL cases). Average payment in those cases was $432,000; five percent of cases closed with $1M+ payments.
In general, clinicians should avoid “defensive” documentation, but there are steps in the documentation process that benefit both the patient’s care and the defensibility of that care if it is later questioned via malpractice claim or lawsuit. Expanded patient access doesn’t mean you have to dramatically alter how and what you chart, but you will want to be sensitive to terminology and descriptive language that may be unnecessarily hurtful or confounding to a lay reader. When unsure, a good rule of thumb is to mirror in your notes the way that you would speak with a patient in person. Specific language that is required for billing and coding should not be altered.
On its website, CRICO has published answers to frequently asked questions about how these new rules and regulations impact patient safety and provider liability. This page also offers the opportunity to pose questions to our MPL and Patient Safety experts.
Many other organizations—in particular, the OpenNotes movement—have developed advice and recommendations for writing “open” notes and managing patient questions and concerns. These include:
- How to write an open note (OpenNotes)
- Information Blocking Resource Center (ACP | AHIMA | AMA | AMIA | APA | CHIME | MGMA | Premier Inc.)
- How do I comply with info blocking (AMA)
Additional Material
Latest News from CRICO
Utilization of Electronic Health Record Sex and Gender Demographic Fields: A Metadata and Mixed Methods Analysis

Establishing a Regional Registry for Neonatal Encephalopathy: Impact on Identification of Gaps in Practice

A Comparative Analysis of Nurse Practitioner, Physician Associate, and Physician Malpractice Risk
