Newsletter
Tracking Trends in Neonatal Encephalopathy Care and Treatment
Mar 31, 2024
A woman in her early twenties was induced 40 weeks into her pregnancy. The medical record noted prolonged drops in the fetal heart rate that responded positively to scalp stimulation, but this note was later crossed out and marked as an error.
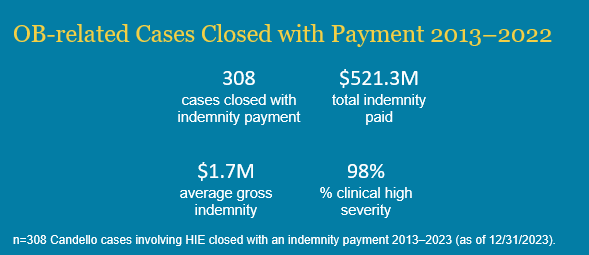
After being delivered vaginally, the baby had low Apgar scores and she was diagnosed with hypoxic-ischemic encephalopathy (HIE). The child is now legally blind, suffers from seizures and has spastic quadriparesis, among other health conditions. After a malpractice claim was filed, defense experts concluded the standard of care was not met and HIE could have been prevented. The case was settled in the millions.
Hypoxic-ischemic encephalopathy presents a formidable challenge in neonatal medicine. The brain injury, caused by a lack of oxygen to the brain before, during, or shortly after labor, often precipitates profound neurological disability or mortality in affected newborns.
As many prenatal and perinatal factors can lead to the condition, HIE itself is not an indication of malpractice. The diagnosis and devastating effects, however, can prompt a case review to assess whether there was a deviation in the obstetrical standard of care. But the groundbreaking treatment of therapeutic hypothermia has proven to prevent further ischemic injury, offering hope when caring for the most vulnerable of patients.
Therapeutic hypothermia limits the extent of brain injury by using a specialized thermometer-controlled blanket to cool an infant’s body temperature down to 33.5 degrees Celsius for three days following delivery.
But the primary obstacles to therapeutic hypothermia treatment are resources and time. To be effective, the treatment must be initiated within six hours of birth for infants with moderate to severe HIE, and only certain neonatal intensive care units (NICUs) have the equipment and specialists available. To expand equitable access to this critical treatment, CRICO awarded grant funding to Boston MedFlight to install active cooling therapy as a standard feature for all neonatal transports. If a neonate needs treatment but it is not available at the hospital where they were born, the cooling treatment can come to them.
Another concern in neonatal cooling therapy is variations in screening and cooling practices across institutions. Aiming to standardize practices, the Academic Medical Center Patient Safety Organization (AMC PSO) convened clinical experts in 2016 and disseminated recommendations to standardize the selection of eligible infants and the administration of therapeutic hypothermia.
To identify variations in therapeutic hypothermia practice and learn more about patients with neonatal encephalopathy, CRICO, the medical malpractice insurer of the Harvard medical community, partnered with 14 institutions in Massachusetts to build a regional neonatal encephalopathy registry.
The registry tracked 502 newborns evaluated for therapeutic hypothermia between 2018 to 2020, with roughly half receiving cooling treatment. The team found variations in cooling and screening practice, demonstrating the need to produce consensus guidelines on what the best practices are when it comes to therapeutic hypothermia. The collaborative also found implementing a regional neonatal encephalopathy registry was feasible and made data collection tools public for other groups to adopt.
While the journey towards optimal management of neonatal encephalopathy may be multifaceted, collective dedication, collaboration, and innovation can improve outcomes for newborn patients and their families.
Additional Material
- Hypoxic-ischemic Encephalopathy (HIE): Symptoms
- Establishing a Regional Registry for Neonatal Encephalopathy: Impact on Identification of Gaps in Practice
- Cooling Brain-injured Babies to Reduce Disability, Liability
- Hypoxic-ischemic Encephalopathy | National Institute of Neurological Disorders and Stroke
Clinical Perspective
Featured on CRICO’s Safety Net podcast: Newborn Body Cooling Safety and Efficacy Moves Forward
“As a neonatologist who’s been taking care of babies for more than 30 years at Boston Children’s Hospital, it’s a wonderful thing for me to see that we now have an intervention which can help the outcomes of babies who have hypoxic-ischemic encephalopathy. For many decades all that we could offer babies and their families was supportive care and with the advent of therapeutic hyperthermia, we have an intervention which we know will improve their outcomes.”
Anne Hansen, MD, MPH
Medical Director, NICUBoston Children’s Hospital
Recent Issues
No Surgical Items Left Behind

Aha!
