Newsletter
Getting to the Detail Devils
Apr 25, 2023
Although the origin of the expression, “the devil is in the details” is foggy, its meaning is clear. Complex concepts comprise numerous components, and any one thing can raise hell. Understanding where to focus finite patient safety resources requires understanding the risk of harm at a detailed level.
Among the more effective approaches to understanding specialty or organization-specific patient safety risks and medical malpractice liabilities is analyzing case types. For medical professional liability (MPL), case type is captured by the allegation codes. Those allegations are, in general, determined by the claimant; it is what they contend led to their injuries and demand for compensation.
Candello uses more than 90 allegation codes (from Administration of the wrong medication dose to wrong/unnecessary treatment/procedure), rolled up into 25 subcategories. While 90 percent of all MPL cases (and 88 percent of potential losses) are captured by 18 of those codes, the level of specificity afforded by having 93 codes to choose from means that coders, analysts, and quality and safety leaders can delve into some clearly defined risks—especially when allegation data is paired with responsible service and contributing factors.
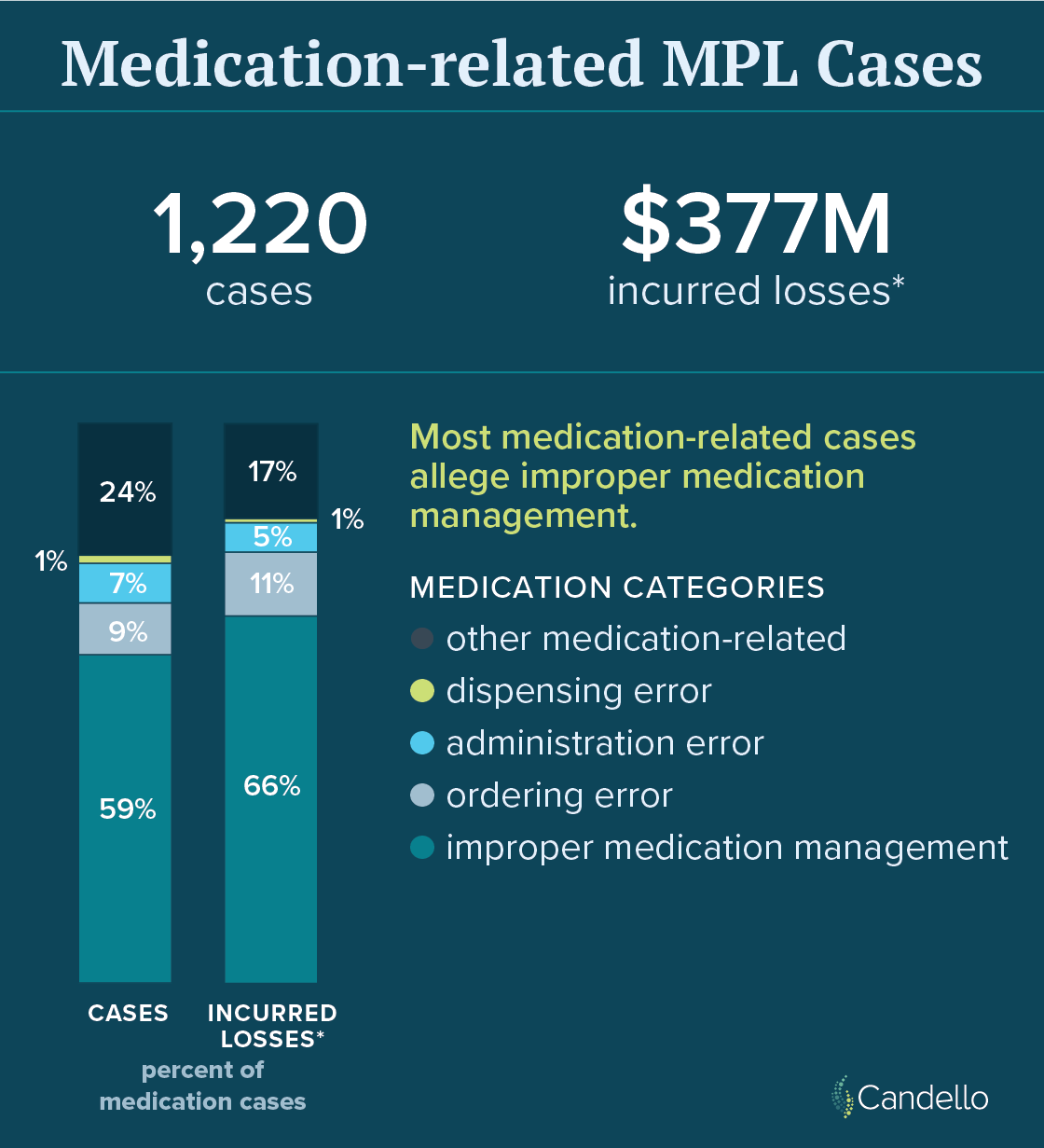
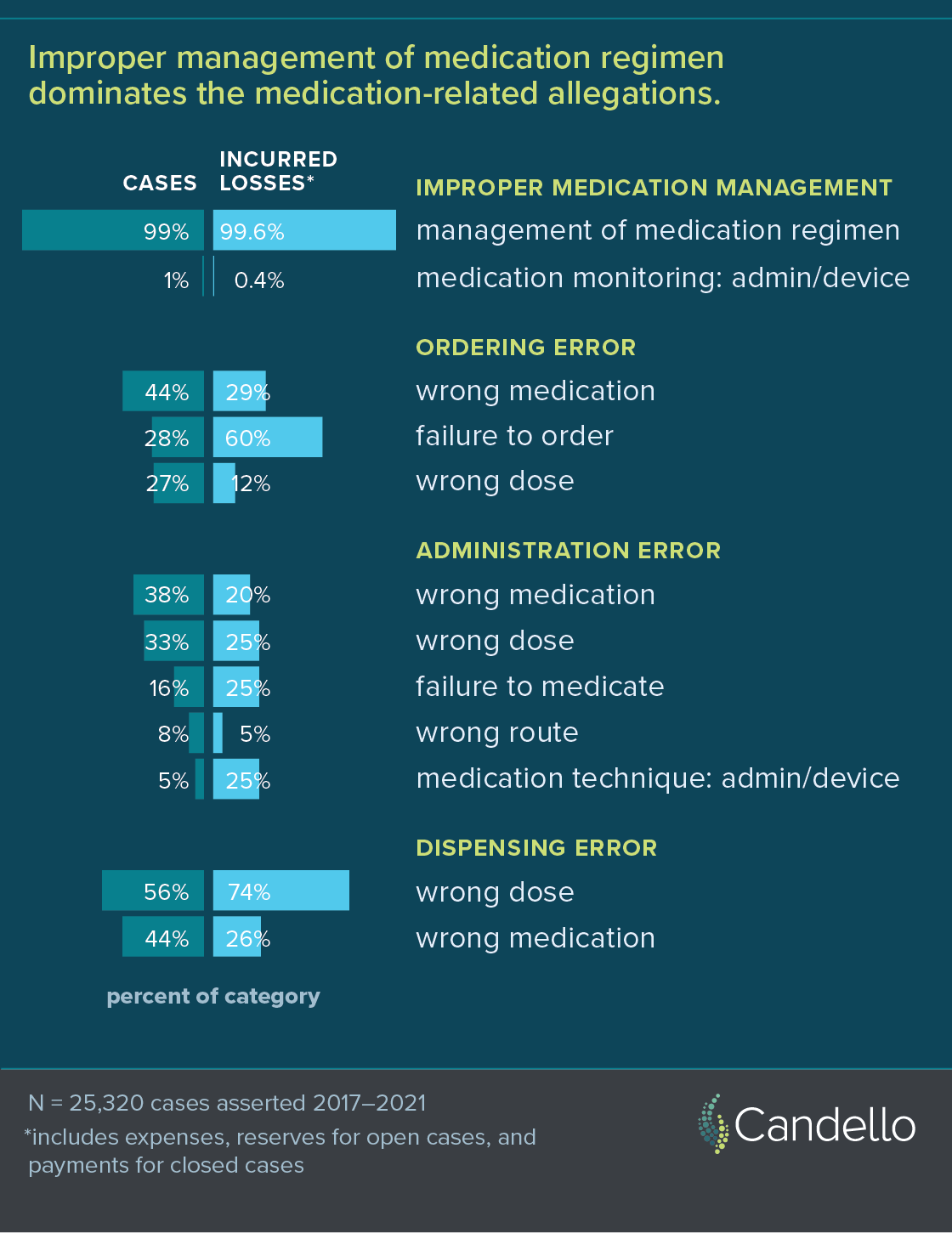
For example, it may be helpful to know that 4.8 percent of 25,320 MPL cases asserted from 2017-2021 were medication related, representing 4.2 percent of the total incurred losses ($377M). It is more helpful to know that fewer than 20 percent of those cases involved drug ordering, dispensing, or administering errors—and that more than half of the MPL cases derived from mismanagement of the patient’s medication regimen. Overall, Candello uses 13 different medication-related allegations to help guide system improvement, which will be quite different for regimen mismanagement than for dispensing errors. Similarly important distinctions are found in allegations related to obstetrical care, surgical treatment, and surgical treatment cases, which at a high-level represent large proportions of MPL cases where being able to pinpoint specific vulnerabilities enables more precisely targeted intervention.
At an individual hospital or service area with small numbers of MPL cases on an annual basis, case type specificity may not be needed to inform those who are aware of those few events, but it can help other health care providers understand why systems improvement is needed and why interventions are being enacted. And those are important details.
Recent Issues


The Diagnostic Multiverse
An MPL Perspective on the SafeCare Study