Newsletter
Exploring the “Allegation” of Medical Malpractice
May 31, 2018

Every medical malpractice claim or lawsuit states or implies an allegation of negligent or substandard care. The allegation frames the plaintiff’s connection between the health care the patient expected and an adverse outcome of that care.
For every MPL case entered into CRICO’s national Comparative Benchmarking System (CBS), the clinical coding specialist must assign a major allegation that best identifies the plaintiff’s complaint. Depending on the source of the malpractice claim or lawsuit, the plaintiff’s allegation may be clearly stated, implied, or obscured by a focus on individuals or tangential interactions rather than the clinical scenario. The coding specialists strive to assign a specific allegation that will help the defendant and the medical professional liability insurer clarify the claimant’s argument, an essential step toward understanding where to begin any investigation into the events in question.
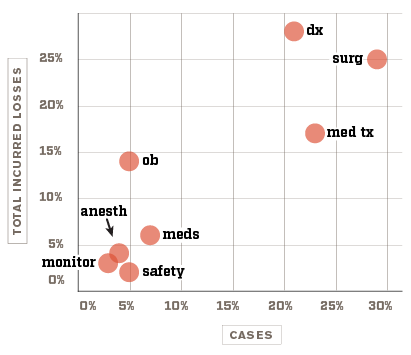
Top Allegations in MedMal Cases
|
Allegation Category |
Abbrev |
Cases |
Total Incurred Losses* |
|---|---|---|---|
|
Surgical Treatment |
surg |
29% |
25% |
|
Medical Treatment |
med tx |
23% |
17% |
|
Diagnosis-related |
dx |
21% |
28% |
|
Medication-related |
meds |
7% |
6% |
|
Safety & Security |
safety |
5% |
2% |
|
Obstetrics-related |
ob |
5% |
14% |
|
Anesthesia-related |
anesth |
4% |
4% |
|
Patient Monitoring |
monitor |
3% |
3% |
*Includes reserves on open cases and indemnity paid for closed cases.
Within the allegation categories, the coding specialists have a set of specific major allegation types by which they can define a case, as well as secondary allegation types they can include when appropriate. The top 10 specific allegations—which account for 75% of cases and 81% of incurred losses—are described below. (Note that the diagnosis-related category has only one allegation choice.)
|
Category |
Allegation |
Cases |
Total Incurred Losses* |
|
Diagnosis-related |
a missed, delayed, or wrong diagnosis illness or injury that results from a missed, delayed, or incorrect diagnosis |
21% |
28% |
|
Surgery-related |
improper performance of surgery technical missteps during a procedure that occurred within an operating room or ambulatory surgery site (excludes anesthesia-related errors) |
17% |
13% |
|
Surgery-related |
improper management of a patient undergoing surgery non-procedural mismanagement of the patient on a surgical path in the pre-op, intra-op, or post-op phase |
9% |
11% |
|
Medical Treatment |
improper management of a patient's treatment course issues related to the care of a patient during the health care delivery process |
8% |
8% |
|
Medical Treatment |
improper performance of a treatment regimen or procedure technical missteps occurring during a procedure outside the operating room or ambulatory surgery site |
10% |
6% |
|
Obstetrics-related |
delay in treatment of fetal distress delay in recognition and/or treatment of a fetus in distress |
1% |
5% |
|
Medication-related |
improper management of a patient's medication regimen failure of any provider to prevent (known) drug interactions or adverse drug events due to inadequate monitoring |
3% |
4% |
|
Obstetrics-related |
improper management of pregnancy issues related to the care and treatment of the mother and/or baby in the antepartum period |
1% |
2% |
|
Patient Management |
failure to monitor the patient's physiological status failure to properly observe and act on changes to the patient's physical status while receiving care, e.g., changes in skin integrity, (ulcer), IV infiltrate, issues related to compression stockings |
2% |
2% |
|
Safety & Security |
failure to ensure safety (falls) failure to prevent patient from falling while in the care of a provider (inpatient or outpatient setting) |
3% |
2% |
*Includes reserves on open cases and indemnity paid for closed cases.
As with any exploration of medical malpractice data, a data source large enough to generate credible evidence is key to being able to illustrate the distribution of cases across various domains. Allegation type is a valuable tool for understanding what aspects of care are most likely to trigger claims of malpractice. Drilling down into the subtypes of those allegations (e.g., the difference between surgical performance and surgery patient management) is an important next step in guiding your organization’s patient safety attention and resources in the most appropriate direction. Exploration of root causes and implementation of interventions/best practices based on a more detailed understanding of adverse event patterns are more likely to lead to effective patient safety improvements.
Recent Issues
Patient Safety Playlist

