Article
Synthesis and Diagnostic Decision Making in an ED

Physicians and nurses who excel at solving diagnostic problems via teamwork are drawn to Emergency Medicine where individuals working with limited information must rely on each other to divine the best strategy for each patient. Of course, these skills usually are practiced in an environment of steady distraction and disrupted communication. This is a chronic problem for the individuals putting the puzzle pieces together in a frenzied environment.
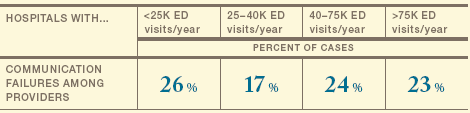
Getting the diagnosis right with minimal delay depends on effective team communication. If Dr. B doesn’t know what Nurse A knows, then Dr. B can’t complete the picture of patient C. Every ED presents at least some of these significant challenges to ensuring that the entire care team has common knowledge:
- an EMR that reduces face-to-face interactions among the ED staff
- a lack of touch-points for providers to synthesize independent bits of knowledge about a patient, especially at changes of shift
- staff that over rely on each other’s habits and tendencies as substitution for asking and confirming
- a lack of sharing subtle changes in a patient’s condition that are noticed, but not noteworthy
Peer-to-peer interactions, clinician-patient discussions, medical record documentation, etc., have to be clear enough to assist contemporary providers and comprehensive enough to guide subsequent caregivers. Organizations that offer training, practice,and support for teamwork skills that enhance clinical decision-making can minimize the risk of uncoordinated care. Continuous collaboration between physician and nurse leadership that involves front-line workers from all disciplines is likely to be effective in driving sustained safety improvements.
How well are you communicating critical information regarding your patient’s condition?
CASE EXAMPLE: DECISION-MAKING
A 47-year-old male with history of asthma presented to the ED complaining of shortness of breath and chest tightness since the prior day. The initial nursing documentation reports SOB episodes consistent with asthma symptoms and a pulling pain in the chest with deep breaths. They also referenced a recent history of a pulled calf muscle one week prior, with bruising and swelling, and a positive Homan’s sign. The attending physician noted the patient was alert, fully oriented, and in no acute distress. The patient also reported recent exposure to new cleaning products at work.
Without scrolling further down in the electronic medical record to view the nurse’s note, the physician ordered no further studies,diagnosed the patient with asthma exacerbation, and discharged him with instructions to use his inhaler at home. The following day,the patient was found dead at home, secondary to massive bilateral pulmonary embolism. (Case settled: $315K).
This page is an excerpt of the full Candello report: Malpractice Risks in the Emergency Department.
ED Benchmarking Report Landing Page