Blog Post
Patient Safety and ‘Off-hours’ Clinical Care

Practicing as a hospitalist at a large academic medical center, I recognize that one of the (many) ways in which I am fortunate is that I have access to on-site specialists any time, day or night. If I have a patient with bleeding around the brain, I know that a neurosurgery resident is available—even in the middle of the night—to come to the bedside, provide consultation, and perform a neurologic exam alongside me as we decide about next steps in the care of the patient.
These types of resources are not typical, and limited availability of specialists is just one of the challenges that clinicians encounter when they are working overnights or on weekends—that is, “off hours.”1 Other challenges that increase the risk of medical errors for clinicians working off hours include being less familiar with the patients (if their care is being directed mainly by the day team), the fatigue associated with working overnight, and, in teaching hospitals, less supervision of resident physicians by more senior attending physicians.
Medical malpractice claims provide a valuable lens through which to evaluate potential patient safety vulnerabilities, such as the risk associated with off-hours medical care. Candello—the database of malpractice claims maintained by CRICO, which includes approximately one-third of U.S. malpractice claims—allows one to drill down to examine important patient safety issues. The claims in the Candello database are manually reviewed by experienced nurse coders, who document various attributes of the case—including the clinician types and specialties involved, as well as the contributing factors underlying the adverse event. Among all the malpractice cases in Candello closed from 2014 to 2018 (numbering more than 38,000), we looked for cases that had a contributing factor of care occurring on a weekend, holiday, or overnight, and investigated whether cases with this contributing factor were more likely to close with a payment being made to the claimant, compared to cases without this contributing factor.
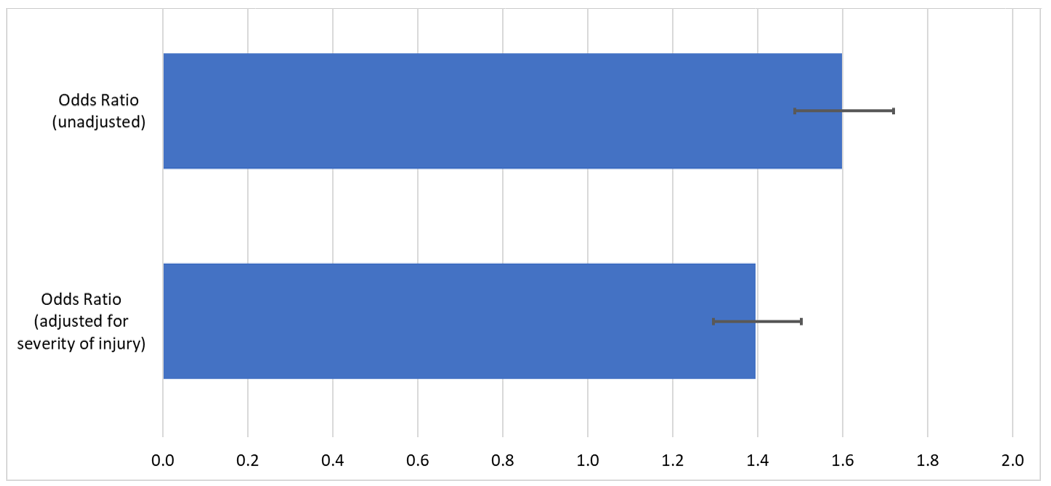
Our analysis showed that malpractice claims in which off-hours care was a contributing factor were indeed significantly more likely to close with a payment being made to the claimant, with an odds ratio of 1.60 (95% confidence interval [CI]: 1.49–1.72). The severity of the patient’s injury is a powerful predictor of any case closing with payment. Therefore, we controlled for injury severity, to see if off-hours care remained significantly associated with a case closing with payment, and it did: with an odds ratio of 1.40 (95% CI: 1.30-1.50). This finding, that off-hours care makes a claim more likely to close with payment, even when controlling for severity of injury, shows that this is a factor to which patient safety officials should pay attention.
Identifying a patient safety vulnerability, such as providing care during off hours, should prompt consideration of actions to make care under such circumstances safer. One way to increase specialist availability during off hours so that clinicians at smaller hospitals can access the expertise they need, when they need it, is to provide consultation via telemedicine. Neurosurgery consultation via telemedicine is being used to provide neurosurgical input, even when there is no on-site neurosurgeon.2,3 We can expect to see increasing use of telemedicine consultation, as the COVID-19 pandemic has helped increase the acceptance of telemedicine across a broad range of clinical settings. Telemedicine neurosurgical consultation for patients with certain conditions, such as subdural hematomas (bleeding around the brain), can provide another advantage—avoiding unnecessary inter-hospital transfers. When patients present with subdural hematomas, they are typically transferred to medical centers with on-site neurosurgery coverage. Neurosurgery consultation via telemedicine can help determine which patients need to be transferred—generally those patients who are more likely to require neurosurgery in the short-term—and which patients can remain at their current hospital with close monitoring.3 This more precise deployment of neurosurgery resources is especially important now, when hospitals across the country are facing unprecedented demands on their capacity.
Additional measures that can be considered to make off-hours care safer include improving how information is transferred from the day team to the night team, and, at academic medical centers, enhancing the supervision of resident physicians. Using systematic approaches to handing off patients from the day team to the night team—including specifying specific action items that need to happen and discussing how to handle contingencies—has been shown to reduce medical errors.4 A reluctance by residents to contact their supervising attending physicians for guidance when a patient becomes sicker, especially when this occurs off hours, can be a barrier to providing the safest possible care. Specifying situations in which the resident is required to contact the attending, such as when a patient requires transfer to the ICU, is one way to counteract this hesitance to seek guidance from more senior physicians.5
One recent development in how inpatient care is provided, especially on internal medicine services, is the increasing use of nocturnists, who are attending physicians that focus on providing care to hospitalized patients overnight. Primarily tasked with providing direct patient care, nocturnists are an underutilized resource when it comes to supervision of resident physicians. As attending physicians who are on site overnight, nocturnists are well positioned to provide supervision of residents who are admitting and covering patients during this time.6,7 However, for such supervision to be effective, it must be in lieu of some portion of the nocturnists’ direct patient care responsibilities, rather than an additional responsibility. By helping identify patient safety issues, and providing methods of quantifying the magnitude of these issues, malpractice data is an important tool that helps promote patient safety, including for off-hours care.
References:
- Shulkin DJ. Like night and day—shedding light on off-hours care. New England Journal of Medicine. 2008;358(20):2091–2093.
- Eichberg DG, Basil GW, Di L, et al. Telemedicine in neurosurgery: Lessons learned from a systematic review of the literature for the COVID-19 era and beyond. Neurosurgery. 2020;88(1):e1–e12.
- Wright J, Elder T, Gerges C, et al. A systematic review of telehealth for the delivery of emergent neurosurgical care. Journal of Telemedicine and Telecare. 2021;27(5):261–268.
- Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. New England Journal of Medicine. 2014;371(19):1803–1812.
- ElBardissi AW, Regenbogen SE, Greenberg CC, et al. Communication practices on 4 Harvard surgical services: A surgical safety collaborative. Annals of Surgery. 2009;250(6):861–865.
- Catalanotti JS, O'Connor AB, Kisielewski M, Chick DA, Fletcher KE. Association between nocturnist supervision and perceived overnight supervision adequacy among internal medicine residents in the US. JAMA. 2020;323(14):1407–1409.
- Haber LA, Lau CY, Sharpe BA, Arora VM, Farnan JM, Ranji SR. Effects of increased overnight supervision on resident education, decision-making, and autonomy. Journal of Hospital Medicine. 2012;7(8):606–610.
Related Blog Posts
Investing in Patient Safety


Mind the Gaps: Learning How to Avoid Miscommunication Pitfalls
January Safety Salute | MedStar Health Creating a Just Culture
