Newsletter
When a Procedure is Anything but Routine
Dec 19, 2013

A nurse’s incorrect selection of needle size for the chemotherapy port results in excoriation of tissue, infection, and the need for additional surgery.
When her care team fails to diagnose a bowel perforation after a screening colonoscopy, the 66-year-old patient dies.
A patient undergoing a core needle biopsy for a breast lesion experiences a lung puncture.
Each year, thousands of patients undergoing routine screening, diagnostic, or therapeutic procedures in an ambulatory care setting face the consequences of a seemingly benign process that went wrong. When those patients are injured and they (or their families) seek compensation for their losses, their physicians, nurses, and technicians have to face the consequences of a medical malpractice allegation.
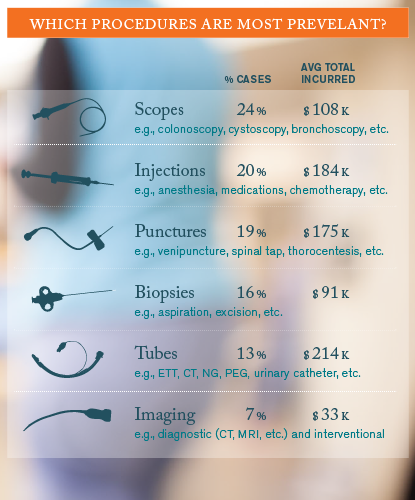
A study of more than 18,000 cases in CRICO Strategies’ national Comparative Benchmarking System (CBS) found that 18 percent (1,497) involved errors related to routine (non-surgical) procedures. The vast majority (71 percent) occurred in ambulatory settings. While more than two thirds of the injuries were relatively minor, 14 percent of the procedure cases involved patients who died. Of the procedure-related cases that have closed, 36 percent closed with a payment (average=$212,000). Most of the procedures that triggered these cases fall into one of six distinct categories:
More than half (56 percent) of the procedure-related cases in the CBS study named a physician (across more than 40 specialties); six percent named a nurse. Although technical errors during the procedure dominate these cases (88 percent), they do not exclusively reflect hands-on skill lapses. Errors related to rules of practice or protocol (21 percent of the cases), and errors in the caregiver’s knowledge and clinical judgment (28 percent) are also commonly involved—often compounding a skill error.
Additional data, case examples, and recommendations and best practices related to routine medical procedures, can be found in Candello’s 2013 Annual Benchmarking Report, Malpractice Risks of Routine Medical Procedures.
This page is an excerpt of a full issue of Insight.
CME: The Massachusetts Board of Registration in Medicine has endorsed each complete issue of Insights or 30-minutes of podcast episodes as suitable for 0.5 hours of Risk Management Category 1 Study in Massachusetts. You should keep track of these credits the same way you track your Category 2 credits.Recent Issues

Who’s Who in Health Care?

A First Place Mindset About Medical Error

Utilization of Electronic Health Record Sex and Gender Demographic Fields: A Metadata and Mixed Methods Analysis


Teleradiology Medical Malpractice Cases